Rawa Ismail: Bridging marketing authorization studies with real world data
Project of Rawa Ismail, PhD candidate at the MEB and DICA
Within the context of my PhD research, a collaboration between the MEB and the Dutch Institute for Clinical Auditing (DICA) is realized. DICA is a not-for-profit organization that facilitates the development and maintenance of national outcomes registries around medical conditions. DICA has established over 20 registries on mainly surgical and oncological conditions, such as melanoma, lung cancer and colorectal cancer. Real world data are collected in the registries to improve quality of care, by mainly doing research with these data.
The data used in this research project are collected in the Dutch Melanoma Treatment Registry (DMTR). In the past years, multiple new immunotherapies and targeted therapies are authorized for the treatment of melanoma patients. These treatments are registered in the DMTR and show a prolonged overall-survival in melanoma care, which was also shown in marketing authorization studies. However, patients and treatment lines used in daily practice differ from the randomized controlled trials, because of the homogenic study population and treatment.
Therefore, the focus of my research will be on the differences in effectivity and toxicity of immunotherapy and targeted therapy between marketing authorization studies and the real-world data collected by DICA in the treatment of melanoma. For example, one of the questions will focus on the patient- and tumour characteristics of long-term survivors on BRAF- and MEK-inhibitors. In another project re-challenge with targeted therapy will be investigated. This kind of information is limited in RCTs, while the heterogenic real-world population is registered in the DMTR. This real-world evidence could be helpful in future scientific advices and in the assessments of similar medicinal products by the MEB.
Yvette Weesie: Opioid prescriptions in primary care
It probably hasn’t escaped anyone’s attention that Western countries are faced with a large increase in opioid use. The United States of America is the most recognized example of problems associated with this increase that has serious societal consequences, like addiction and increased opioid related mortality. The so-called opioid epidemic in the USA triggered other Western countries to take a serious look at the development of opioid use within their own borders. So did the Medical Evaluation Board (MEB) in the Netherlands, who asked me and my colleagues at Nivel (Netherlands institute for health services research) to capture the prescribing of opioids of Dutch general practitioners (GP’s).
We studied the trend of opioid prescriptions in the period 2005 to 2015. Like other countries, the Netherlands shows a large increase in the prescription of opioids, especially when it comes to strong opioids. We found a six fold increase in number of patients being prescribed a strong opioid, such a oxycodone. We also found that opioids are mainly prescribed for non-cancer related diagnoses of which musculoskeletal diagnoses are the number one diagnoses. The proportion of chronic use was constant between 2005-2015 at approximately 30% of the patients. On the 5th of June 2019 I will present an updated version of this study at the “CBG Collegedag” in a workshop on good use of opioids. Also my first article about opioid prescriptions to elderly patients in primary care has just been submitted.
Our study for the MEB provided new insights and causes for action. Still, many aspects of opioid prescribing are unknown. For instance; who initiates the opioid prescription, the GP or the specialist? What is the variation in opioid prescription between GP-practices? What do GPs think about the current developments around opioids? And how do GPs prescribe opioids to patients who are more at risk for adverse effects or fall-related injuries, like the elderly? Can we constantly monitor prescribing of opioids? With my PhD-research we will try to answer these questions by looking at the prescription of opioids, with a focus on the primary care setting.
Our Nivel Primary Care Database, containing data from 500 general practices, 33 out-of-hours GP services and 124 physiotherapy practices, is an excellent basis for research. We can match prescriptions with information on the diagnoses for which they are prescribed. We have longitudinal information of patients electronic health records. With this information we are in the unique position to follow patients over the years and we can zoom in on treatments with specific diagnoses. Also, we can match our GP data with data of physiotherapists and that of out-of-hours GPs. As such we can follow patients care paths during their treatment with opioids. Finally, in half of the 500 practices that participate data are extracted weekly, meaning that we can monitor opioid use almost real-time. Thus, with my PhD-research, I hope to provide useful information as a basis for policy and interventions in clinical practice.

Noëlle Lugtenburg: Design for interaction
My name is Noëlle Lugtenburg. I am a master student Design for Interaction at Delft University of Technology (TU Delft). In my studies I learn to design products and services for people to be used during daily lives, from the perspective of the user. By doing user research and by understanding their lives, needs, capabilities and motivations, I have learned to design products that are relevant to the user and fit their needs.
For my graduation I got the opportunity to work on a project for the Medicines Evaluation Board (MEB), within the Better Use programme, in collaboration with the VUmc Department of Obstetrics and Gynaecology. The goal of my project is to design a new product with information about medicines for pregnant women. This project contributes to MEB’s goal to improve accessibility and understandable information provision about medicines for patients.
Research into patient needs
The project consists of two parts; the research phase and the design of the product. The first step was to obtain understanding of the current situation, by doing literature research into medication use among pregnant women, medication (non)adherence (which is a problem among pregnant women), risk perception & communication and already existing sources of information on medicines. This gave insight into problems with current medication information sources and provided initial requirements for the design of a new product.
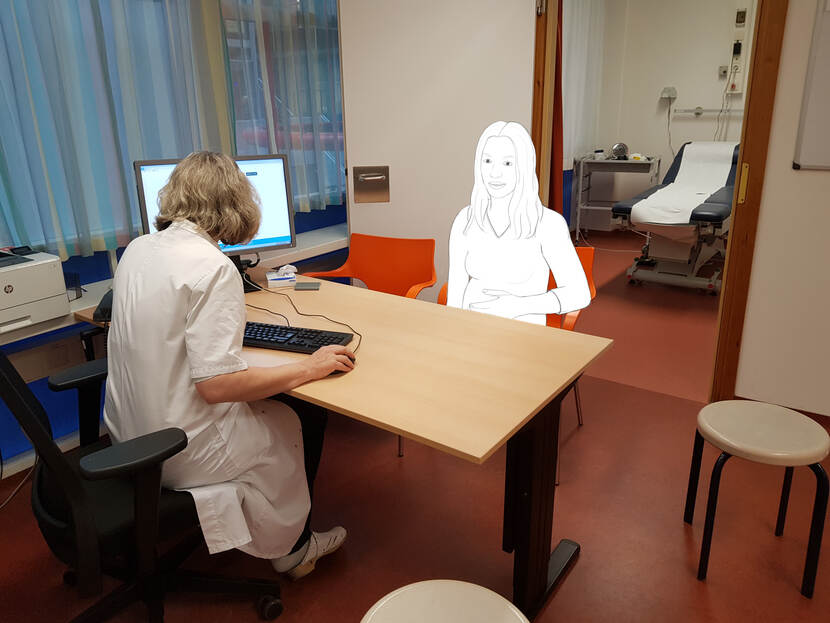
As a designer it is always important to get a good understanding of the user(‘s needs) and the context you are designing for. To better understand the clinical practice and the interaction between prescriber and patient, I have observed several consultations of pregnant women with gynaecologists at VUmc. Next to this, the user research was conducted. This included nine interviews with pregnant women that were treated in VUmc and used one or more medicines. The aim was to get insight into their experiences and needs regarding information about medication that helped to identify further requirements for the design.
One of the main findings of the research phase was that pregnant women are afraid that medicines may harm their unborn child and therefore they need to receive information about the risks of medicines for their child when they use it during pregnancy. On the other hand, it became also clear that not using a medicine may sometimes also be harmful for mother and/or child, which could be important information to share as well. Moreover, the benefits of medicines for the pregnant women and their child require more attention in the provided information. These are usually explained by the prescriber but only very limited in existing information on medicines. Based on this it was concluded that the benefits and risks of medicines used during pregnancy should be presented in a balanced way.
Designing an app
Based on all research insights, I formulated a design goal and vision on how the interaction between patient and product should be. The design process started with generating ideas through multiple creative sessions, eventually resulting in a final concept. The final product, which I am currently working on, is an app that provides balanced information about benefits and risks of medicines, including the risks when not using the medicine, and communicates relevant, compact and understandable information in a user friendly way. By using a prototype of the app, I am planning to do an evaluation test with pregnant women to see whether the design meets the requirements and patients needs. Hopefully my design will be one step forward in improving the medication information for pregnant women.
See the full overview of PhD projects in Regulatory Science with involvement of the MEB